Coronary artery bypass grafting (CABG) has come full circle-it started as an off-pump affair, then became an on pump one and now we are trying to keep off the pump again. One of the main reasons for this has been the neurological sequelae subsequent to CABG. But neurological problems kept causing concern even in off-pump CABGs (OPCAB). Side clamping the aorta was thought to be the major factor and thus came the concept of ‘no touch proximal anastomoses’ onto the aorta (1). Though a variety of proximal anastamotic devices are available in the market, high cost is a matter of real concern in third world countries like India. Hence, this endeavor of ours to fabricate an anastamotic device of our own-‘the Vettath’s anastamotic obturator’ (VAO) for proximal anastomoses of saphenous vein grafts (SVG) onto the aorta. VAO is a stainless steel rod with three grooves and a guard at the end, which sinks into the aorta, through a punch hole, cordoned off by two wide purse string sutures.
VAO can be employed for both on pump and off pump Redo-CABG. The approach is through median sterno- tomy. It is universally observed that the proximal stump of even totally occluded vein grafts are soft and offer an ideal site for placing top ends of new vein grafts. These sites are identified. After completing distal anastomoses, a 3-0-polyprolene purse-string suture is placed around the intended site of top end anastomosis and it is snared. A No.11 knife is used to make a stab incision in the center of the purse- string suture. This hole is occluded with the left index finger and punched out using a 4.5 mm aortic punch. This site is again covered with left index finger to prevent bleeding. Then the VAO is inserted into the punch hole and the snare is tightened just enough to prevent bleeding. The proximal end of the vein graft is then sutured to the new punch hole using 5-0-polypropylene suture using the technique already described. The same technique could be used to perform 2 or 3 top ends. Another similar circumstance where a side clamp on aorta is better avoided is in combined aortic valve surgery and CABG. Here, the presence of calcium on aortic wall or the need to avoid crushing the aortic suture line necessitates the use of VAO, if the surgeon intends to perform the top end after release of the cross clamp for want of space in short ascending aortic patients. The proximal end of vein graft is connected to the aorta using the aforementioned technique after removal of cross- clamp.



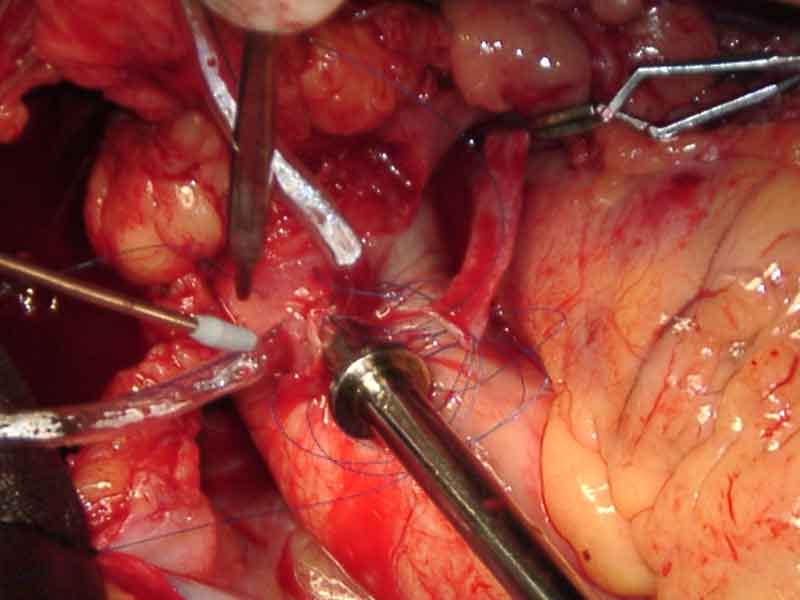
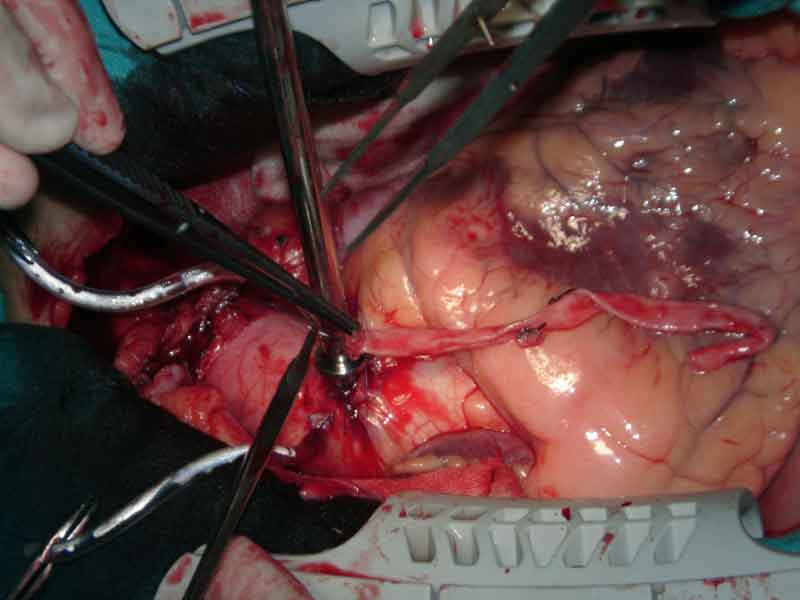
Vettath Anastomotic Obturator being performed on Beating Heart
PUBLISHED ARTICLES
Extended Use of Vettath’s Anastomotic Obturator (VAO) http://file.scirp.org/Html/8453.html
VETTATH’S ANASTOMOTIC OBTURATOR — OUR EXPERIENCE OF 269 PROXIMAL ANASTAMOSIS. https://doi.org/10.1016/j.hlc.2004.02.019
VETTATH’S ANASTOMOTIC OBTURATOR-OUR EXPERIENCE OF 269 PROXIMAL ANASTAMOSIS. Mims Heart Journal, Vol.2, April 2004
Vettath’s Anastomotic Obturator: A Simple Proximal Anastomotic Device http://journal.hsforum.com/index.php/HSF/article/view/1138